
What is it for ?
This website describes the pharmacokinetic and pharmacodynamic interactions between medicines and illicit drugs in order to maintain the efficacy of medicines and avoid adverse effects.
Name/acronym/symbol
Cigarette/cigar/smokes/snus/snuff/pipe
Form and method of administration
Leaves/gum - Smoked/chewed
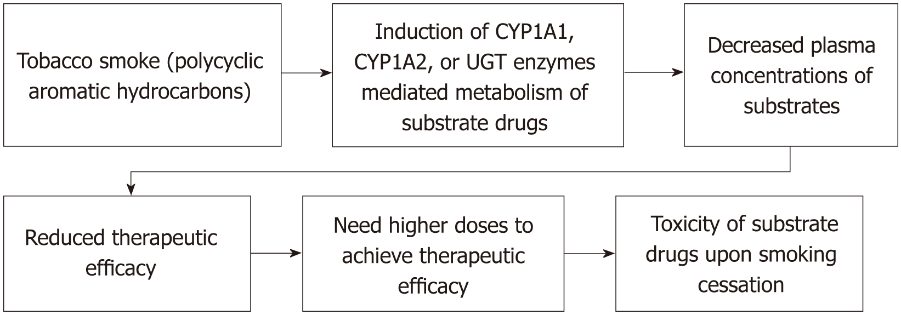
Pharmacokinetic properties
Major inductor of CYP450 1A1, 1A2, 2E1
Nicotine: primarily metabolized by CYP2A6 into cotinine
| 1A1 | 1A2 | 2E1 | |
|---|---|---|---|
| Inducer |
| Major metabolic pathway / potent inhibitor-inducer | |
|---|---|
| Minor metabolic pathway / moderate inhibitor-inducer |
Pharmacodynamic properties
Nicotinic acetylcholine receptors (nAChR) agonist
Central nervous system stimulant
Transient tachycardia, cutaneous vasoconstriction, and a rise in blood pressure
Increase tone and contractility of the gastrointestinal tract
Associated with ischemic heart disease.
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Aminophylline Theophylline | 1A2 and 2E1 substrates. Reduced plasma levels | Increasing of plasma levels | High | When quitting smoking, the theophylline dose may need to be reduced by 25-33% within one week. Conversely, if a patient starts smoking, an increase in the dose may be necessary, as smokers often require higher maintenance doses. |
| Clozapine | 1A2 (and 3A4) substrate. Reduced plasma levels | Increasing of plasma levels | High | Enhanced pharmacological monitoring (at least weekly) when patient stops smoking, or smoke again after stopping. When quitting smoking, the clozapine dose may need to be reduced by 25% within one week. If a patient start smoking, the clozapine dose may need to be increased by 50%. |
| Erlotinib | 1A2 (and 3A4) subtrate. Reduced erlotinib exposure by 50-60% when smoking. | Increasing of plasma levels | High | Smokers should quit as early as possible before starting treatment. If they stop smoking, reduce erlotinib to the initial dose. For smokers, erlotinib dose may be increased by 50mg every two weeks, up to a maximum of 300mg, the highest tolerated dose for smokers. |
| Olanzapine | 1A2 substrate. Reduced olanzapine levels. | Increasing of plasma levels. | High | When quitting smoking, the olanzapine dose may need to be reduced by 25%. If restarting smoking, increase dose to previous smoking dose within one week. Clinical and pharmacological monitoring. |
| Riociguat | 1A1 substrate. Reduced plasma levels by 50-60%. | Increasing of plasma levels | High | Smokers should quit as early as possible before starting treatment. When quitting smoking, dose may need to be reduced. Patients who smoke or begin smoking during treatment may need a dose escalation to the maximum daily dose of 2.5mg three times daily. |
| Tricyclic antidepressants | Substrates of 1A2 enzyme. Smoking may decrease blood levels | Increasing of plasma levels | High | Monitor for side effects and consider dose adjustment if appropriate. |
| Combined hormonal contraceptives (CHC) | Synergism. Women who smoke and use Combined Hormonal Contraceptives (CHCs) face an increased risk of venous thromboembolism (VTE) as well as ischemic stroke and myocardial infarction (MI). CHCs administration is contraindicated in women over 35 years who smoke more than 15 cigarettes a day. | - | High | Women who smoke and use Combined Hormonal Contraceptives (CHCs) are advised to quit smoking or consider alternative contraceptive methods, such as progestin-only pills. |
| Hormonal replacement therapy (HRT) | 1A1, 1A2 (and 3A4) substrate. Reduced plasme levels | High | Smoking womens should consider using transdermal HRT. | |
| Flecainide | 1A2 subtrate. Reduced plasma levels by 50-60%. | Increasing of plasma levels | Moderate | Enhanced clinical and pharmacological monitoring. Consider dose reduction when patient stops smoking. |
| Methadone | 1A2 substrate | Increasing of plasma levels | Moderate | If a patient, who takes methadone, stops smoking they should be monitored for signs of methadone toxicity. The dose of methadone should be adjusted accordingly. |
| Warfarin | 1A2 subtrate. Reduced plasma levels | Increasing of plasma levels | Moderate | Routine INR monitoring.. Stay vigilant for potential changes in warfarin dose, in patients who have altered their smoking status. |
| Others 1A2 substrates | Smoking may lower plasma levels | Increasing of plasma levels | Moderate | Association with major substrates of 1A2 is not recommended. Dosage increase may be required if associated. If the patient stops smoking, monitor for adverse effects, dosage reduction may be required. Taken in account when associated with minor substrates of 1A2. Clinical and/or pharmacological monitoring in case of combination. |
| Benzodiazepines (BZD) | Stimulation from nicotine may reduce sedative effect. | Potential increase in levels with smoking cessation Possible increase in sedation. Excessive central nervous system depression may occur when the patients stop smoking. | Moderate | Monitor - may require dosage reductions if smoking is stopped. |
| Antihypertensives | Antagonism. Nicotine increase the sympathetic activity and rises the blood pressure. Less effective antihypertensive and heart rate control. | Potential increase in levels with smoking cessation Antihypertensive Effect may be enhanced. Possible bradycardia and hypotension. | Moderate | Dosage increase may be required if associated. Monitor - May require dosage reduction if smoking is stopped. |
| Statins | Antagonism. Decrease of statins’s beneficial effects | Increase in beneficial effect on the reduction of morbidity and mortality associated with ischemic heart disease | Moderate | Patients should be advised to stop smoking. |
| Others 2E1 substrates | Smoking may lower plasma levels | Increasing of plasma levels | Moderate | Taken in account when associated with minor substrates of 2E1. Clinical and/or pharmacological monitoring in case of combination. |
| Opioids | Smoking is linked with hyperalgesia due to desensitization of nAChR. | Adequate pain control may be experienced with lower opioid doses | Moderate | The smokers may need higher doses of opioids and the smokers requiring opioid analgesics should be advised to quit smoking. |
| UGT substrates | Unclear data concerning induction of UGT enzymes by PAHs of tobacco smoke | Unknown | Clinical monitoring |
- https://www.hug.ch/sites/interhug/files/structures/pharmacologie_et_toxicologie_cliniques/a5_cytochromes_6_2.pdf
- https://www.rqesr.ca/stock/fra/Drug-InterACTIONS-with-Tobacco-Smoke-FR-9x12-Print-FINAL.pdf
- https://www.health.nsw.gov.au/tobacco/Factsheets/tool-7-guide-dug-interactions.pdf
- http://agence-prd.ansm.sante.fr/php/ecodex/rcp/R0314938.htm
-
(1)
1. Benowitz NL. Pharmacology of Nicotine: Addiction, Smoking-Induced Disease, and Therapeutics. Annu Rev Pharmacol Toxicol. 2009;49:57‑71.
2. Sarparast A, Thomas K, Malcolm B, Stauffer CS. Drug-drug interactions between psychiatric medications and MDMA or psilocybin: a systematic review. Psychopharmacology (Berl). juin 2022;239(6):1945-76.
-
Institute of Medicine (US) Committee to Assess the Science Base for Tobacco Harm Reduction; Stratton K, Shetty P, Wallace R, et al., editors. Clearing the Smoke: Assessing the Science Base for Tobacco Harm Reduction. Washington (DC): National Academies Press (US); 2001. 9, Nicotine Pharmacology. Available from: https://www.ncbi.nlm.nih.gov/books/NBK222359/
-
Pakkir Maideen NM. Tobacco smoking and its drug interactions with comedications involving CYP and UGT enzymes and nicotine. World J Pharmacol. 30 janv 2019;8:14‑25.
-
Maideen NMP. Tobacco smoking and its drug interactions with comedications involving CYP and UGT enzymes and nicotine. World J Pharmacol 2019; 8(2): 14-25 [DOI: 10.5497/wjp.v8.i2.14]
- https://greatermanchester.communitypharmacy.org.uk/wp-content/uploads/sites/118/2023/06/3.-UKMI-Smoking-and-medicines-interactions.pdf
-
van der Plas A, Pouly S, Blanc N, Haziza C, de La Bourdonnaye G, Titz B, Hoeng J, Ivanov NV, Taranu B, Heremans A. Impact of switching to a heat-not-burn tobacco product on CYP1A2 activity. Toxicol Rep. 2020 Oct 29;7:1480-1486. doi: 10.1016/j.toxrep.2020.10.017. PMID: 33204648; PMCID: PMC7649435.
-
Taylor DM, Barnes TR, Young AH. The Maudsley Prescribing Guidelines in Psychiatry 13th edition. John Wiley & Sons; 2018.
-
Buckingham R (ed). Martindale: The Complete Drug Reference [Internet]. London: Pharmaceutical Press. Last updated 10/12/2019 [cited 19/02/2019].
Available from: www.medicinescomplete.com -
Preston CL (ed). Stockley’s Drug Interactions [Internet]. London: Pharmaceutical Press. Last updated 12/11/2019 [cited 19/02/2019].
Available from: www.medicinescomplete.com -
Napp Pharmaceuticals Limited. UNIPHYLLIN CONTINUS 200 mg, 300 mg and 400 mg prolonged release tablets. Last revised 03/2017 [cited 12/05/2020].
Available from: www.medicines.org.uk -
Mylan Products Ltd. Summary of Product Characteristics – Clozaril 25 mg Tablets. Last revised 04/2020 [cited 12/05/2020].
Available from: www.medicines.org.uk -
Generics [UK] Limited t/a Mylan. Summary of Product Characteristics – Erlotinib 100 mg filmcoated tablets. Last revised 02/2020 [cited 12/05/2020].
Available from: www.medicines.org.uk -
Accord Healthcare Limited. Summary of Product Characteristics – Olanzapine Accord 10 mg film-coated tablets. Last revised 09/2015 [cited 12/05/2020].
Available from: www.medicines.org.uk -
Bayer AG. Summary of Product Characteristics – Adempas 0.5 mg film-coated tablets. Last revised 02/2019 [cited 12/05/2020].
Available from: www.medicines.org.uk -
Dr. Reddy's Laboratories (UK) Ltd. Summary of Product Characteristics – Chlorpromazine 100mg Tablets. Last revised 12/2016 [cited 12/05/2020].
Available from: www.medicines.org.uk -
Aurobindo Pharma - Milpharm Ltd. Summary of Product Characteristics – Flecainide Acetate 100 mg tablets. Last revised 01/2018 [cited 12/05/2020].
Available from: www.medicines.org.uk -
Thornton & Ross Ltd. Summary of Product Characteristics – Methadone 1mg/ml Oral Solution BP – Sugar Free. Last revised 04/2015 [cited 12/05/2020].
Available from : www.medicines.org.uk -
Wahawisan J, Kolluru S, Nguyen T et al. Methadone toxicity due to smoking cessation--a case report on the drug-drug interaction involving cytochrome P450 isoenzyme 1A2. Ann Pharmacother. 2011;45(6):e34.
-
Mercury Pharmaceuticals Ltd. Summary of Product Characteristics – Marevan 0.5mg Tablets. Last revised 04/2018 [cited 12/05/2020].
Available from: www.medicines.org.uk -
Jordan SD, Stone MD, Alexander E et al. Patient case: impact of smoking cessation on international normalized ratio. J Pharm Pract. 2014;27(5):470-3. Villard PH, Herber R, Sérée EM, Attolini L, Magdalou J, Lacarelle B. Effect of cigarette smoke on UDP-glucuronosyltransferase activity and cytochrome P450 content in liver, lung and kidney microsomes in mice. Pharmacol Toxicol. 1998 Feb;82(2):74-9. doi: 10.1111/j.1600-0773.1998.tb01401.x. PMID: 9498235.
Name/acronym/symbol
Booze/juice/sauce/hard
Form and method of administration
Liquid
Ingested
Pharmacokinetic properties
Metabolized by alcohol deshydrogenase into acetaldehyde
Major substrate of 2E1
Minor substrate of 1A2 and 3A4
Major inducer of 2E1
We only consider chronic alcohol intake which induces the CYP 450 2E1.
(Occasional consumption inhibits the CYP 450 2E1).
| 1A1 | 2E1 | 3A4 | |
|---|---|---|---|
| Inducer | |||
| Substrate |
| Major metabolic pathway / potent inhibitor-inducer | |
|---|---|
| Minor metabolic pathway / moderate inhibitor-inducer |
Pharmacodynamic properties
Depressive effect on central nervous system.
Mild anxiolytic, disinhibition of behavior, sedation and respiratory depression.
Long-term heavy ethanol use is associated with a persistent increase in diastolic and systolic blood pressure.
Ethanol at high doses also prolongs the QT interval and ventricular repolarization supraventricular tachyarrhythmias, atrial fibrillation, and cardiomyopathy.
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Metformin | Synergism. Alcohol dependence promotes the occurrence of lactic acidosis | - | High | Avoid ethanol consumption in general. If associated, use the minimum effective dose. |
| Neuroleptics | Pharmacodynamic synergism, central nervous system depressant | High | ||
| Benzodiazepins, zolpidem, zopiclone, dextromethorphan, tricyclic antidepressants, antihistamines | Pharmacodynamic synergism, risk of respiratory depression/psychomotor impairment | Potential increase in levels. Sedative effect may be enhanced. | High | |
| Acitretin | Formation of etretinate, a teratogenic metabolite. Contraception for 3 years after treatment cessation. | - | High | |
| Tolbutamide, metronidazole, sulfamides, griseofulvine, disulfiram | Antabuse syndrom | - | High | |
| Paracetamol | Accumulation of NAPQI. Risk of liver necrosis. | - | High | |
| Long acting oral hypoglycemics, methyldopa, hydrazalazine, nitroglycerin | Hypoglycaemia and hypotension | - | Moderate | Not recommended. Clinical and/or pharmacological monitoring in case of combination. Use the minimal effective dose |
| Other minor 2E1 substrates Ethosuximide, everolimus, theophylline | Reduced plasma concentrations which may decrease medication efficacy | Increasing of plasma levels | Moderate | Not recommended. Clinical and/or pharmacological monitoring in case of combination. |
| 1A2/3A4 inducers | Reduced ethanol plasma concentrations which may induce withdrawal symptoms | Increasing of ethanol plasma levels why may induce side effects | Moderate | Clinical/pharmacological monitoring if associated or stopped. |
| 1A2/3A4 inhibitors | Increased ethanol plasma concentrations which may induce side effects. | Reduced plasma levels which may induce withdrawal | Moderate | Clinical/pharmacological monitoring if associated or stopped. |
| Warfarin | Unclear data Heavy drinkers may induce the hepatic metabolism of anticoagulants. However (Lane et al, 1985) : « there was no difference in the magnitude or duration of prolongation of the prothrombin time » | Moderate | Frequent INR and clinical monitoring is recommended |
- https://www.hug.ch/sites/interhug/files/structures/pharmacologie_et_toxicologie_cliniques/a5_cytochromes_6_2.pdf
-
Goullé JP, Guerbet M. Éthanol : pharmacocinétique, métabolisme et méthodes analytiques [Pharmacokinetics, metabolism, and analytical methods of ethanol]. Ann Pharm Fr. 2015 Sep;73(5):313-22. French. doi: 10.1016/j.pharma.2015.03.003. Epub 2015 Apr 7. PMID: 25857743.
-
Fraser AG. Pharmacokinetic interactions between alcohol and other drugs. Clin Pharmacokinet. 1997 Aug;33(2):79-90. doi: 10.2165/00003088-199733020-00001. PMID: 9260032.
-
Chan LN, Anderson GD. Pharmacokinetic and pharmacodynamic drug interactions with ethanol (alcohol). Clin Pharmacokinet. 2014 Dec;53(12):1115-36. doi: 10.1007/s40262-014-0190-x. PMID: 25267448.
-
Addiction Suisse. (2020). Interaction entre l'alcool et les médicaments : informations à l'attention des professionnels du domaine des soins et du travail auprès des personnes âgées. 12 p.
Name/acronym/symbol
Canna/weed/shit/3x/space cakes/Hashish/bang/herb/zedou/Marijuana/skunk/sinsemilla/hash/zamal/pot/dope
Form and method of administration
Green flower or brown resin or golden oil
Smoked most of the time, can be ingested
Pharmacokinetic properties
THC
Δ9- tetrahydrocannabinol (THC) is the main psychoactive compound of cannabis, responsible for the “high” associated with cannabis use.
Major substrate of 2C9 and P-gp
Minor substrate of 3A4
| 2C9 | 3A4 | P-gp | |
|---|---|---|---|
| Substrate |
CBD
Cannabidiol (CBD) is not a psychoactive compound of cannabis.
Major substrate of 3A4 and 2C19
CBD strongly inhibits 3A4, minor inhibition of 1A2
| 1A2 | 2C19 | 3A4 | |
|---|---|---|---|
| Substrate | |||
| Inhibitor |
| Major metabolic pathway / potent inhibitor-inducer | |
|---|---|
| Minor metabolic pathway / moderate inhibitor-inducer |
Cannabis smoked/vaporized result in significant upregulation of CYP1A1 and 1A2.
| 1A1 | 1A2 | |
|---|---|---|
| Inducer |
Pharmacodynamic properties
Sedation
Cognitive and psychomotor impairment, psychotic symptoms, altered perception, increased anxiety
Tachycardia via direct agonism of CB1 receptors
Recommendations :
CANNABIS SMOKED/vaporized = TOBACCO TABLE + Specific pharmacodynamic/pharmacokinetic interactions (down below, except 2E1 substrates)
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Amphetamines, cocaine, atropine ,or other sympathomimetic agents | Additive hypertension and tachycardia | Moderate | Clinical monitoring. Dosages may be adapted | |
| Nivolumab | Combined use with cannabis was associated with a reduction in treatment response rates in patients with advanced melanoma, non-small-cell lung cancer, and renal clear cell carcinoma | Moderate | Association at the discretion of the oncologist depending on the therapeutic objective | |
| Fluoxetine | Case reports of mania resulting from co-administration of cannabis | Moderate | Clinical monitoring. Dosages may be adapted | |
| Disulfiram | Delirium and hypomania resulting from co-administration with cannabis | Moderate | Clinical monitoring. Dosages may be adapted | |
| Sedatives or hypnotics | Sedation and significant pharmacodynamic synergism when taken with cannabis via potentiation of central effects | Moderate | Clinical monitoring. Dosages may be adapted | |
| Warfarin | Induction of metabolism, reduced warfarin levels | Increased warfarin levels | Moderate | Close INR monitoring |
| Clobazam | Induction of metabolism, reduced clobazam levels | Increased clobazam levels | Moderate | Clinical and pharmacological monitoring of clobazam and norclobazam levels |
Oral CBD
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Anti-aromatases | Unclear pharmacodynamic interaction suspected, may reduce anti-cancer medication efficacy. | High | Association at the discretion of the oncologist depending on the therapeutic objective | |
| Letrozole, darolutamide, cyproterone | Possible interaction, may increase anti-cancer treatment plasma levels | High | Possible association. Clinical and pharmacological monitoring. | |
| 2C19/3A4 inhibitors | Increased CBD plasma levels | Reduced CBD plasma levels | Moderate | Clinical/pharmacological monitoring |
| 2C19/3A4 inducers | Reduced CBD plasma levels which may decrease medication efficacy | Increased CBD plasma levels | Moderate | Clinical/pharmacological monitoring |
| Substrates of CYP3A4, especially those with narrow therapeutic index | Increased substrates plasma levels | Reduced substrates plasma levels | Moderate | Clinical/pharmacological monitoring |
| CYP 2C19 substrates | Increased substrates plasma levels | Reduced substrates plasma levels | Moderate | Clinical/pharmacological monitoring |
| Central nervous system depressants (e.g. alcohol, opioids, benzodiazepine receptor agonists,) | Pharmacodynamic synergism. Additive cognitive and psychomotor impairment. | Low | Clinical monitoring | |
| Tamoxifene, abiraterone, enzalutamide, apalutamide, darolutamide, Gn-RH analogs, degarelix | No interaction expected | Low | Possible association. Eventual Clinical/Pharmacological monitoring. | |
| P-gp substrates | CBD may inhibit p-glycoprotein drug transport. | Increased substrates plasma levels | Low | Clinical/pharmacological monitoring for increased substrates toxicity |
Oral THC
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Checkpoint inhibitors -mab immunotherapies | Unclear pharmacodynamic interaction suspected, may reduce anti-cancer medication efficacy. | High | Association at the discretion of the oncologist depending on the therapeutic objective | |
| 2C9 / 3A4 / P-gp inhibitors | Increased THC plasma levels. Risk of increased psychoactive effects. | Reduced THC plasma levels | Moderate | Clinical/pharmacological monitoring |
| Central nervous system depressants | Pharmacodynamic synergism. Additive cognitive and psychomotor impairment. | Reduced psychoactive effects | Moderate | Clinical monitoring |
| Sympathomimetics | Pharmacodynamic synergism. Additive cognitive and psychomotor impairment. | Reduced psychoactive effects | Moderate | Clinical monitoring |
| 2C9 / 3A4 / P-gp inducers | Reduced THC plasma levels which may decrease medication efficacy. | Increased THC plasma levels. Risk of increased psychoactive effects. | Moderate | Clinical/pharmacological monitoring |
| Tamoxifene, anti-aromatases, abiraterone, enzalutamide, apalutamide, darolutamide, Gn-RH analogs, degarelix, cyproterone | No interaction expected | - | Possible association |
- https ://www.hug.ch/sites/interhug/files/structures/pharmacologie_et_toxicologie_cliniques/a5_cytochromes_6_2.pdf
- https ://www.cmaj.ca/content/cmaj/suppl/2020/02/24/192.9.E206.DC1/191097-five-1-at.pdf
- https ://ansm.sante.fr/uploads/2022/04/12/20221412-rapport-gpco-evaluation-des-interactions-cannabis-a-usage-medical.pdf
-
Anderson, G.D., Chan, LN. Pharmacokinetic Drug Interactions with Tobacco, Cannabinoids and Smoking Cessation Products. Clin Pharmacokinet 55, 1353-1368 (2016). https://doi.org/10.1007/s40262-016-0400-9
-
Lucas, C. J., Galettis, P., and Schneider, J. (2018) The pharmacokinetics and the pharmacodynamics of cannabinoids. Br J Clin Pharmacol, 84: 2477–2482. https://doi.org/10.1111/bcp.13710.
-
Casajuana Köguel C, López-Pelayo H, Balcells-Olivero MM, Colom J, Gual A. Psychoactive constituents of cannabis and their clinical implications: a systematic review. Adicciones. 2018 Apr 15;30(2):140-151. English, Spanish. Doi: 10.20882/adicciones.858. PMID: 28492950.
-
Taha T, Meiri D, Talhamy S, Wollner M, Peer A, Bar-Sela G. Cannabis Impacts Tumor Response Rate to Nivolumab in Patients with Advanced Malignancies. Oncologist. 2019 Apr ;24(4) :549-554. Doi : 10.1634/theoncologist.2018-0383. Epub 2019 Jan 22. PMID : 30670598 ; PMCID : PMC6459234.
-
T. Taha, S. Talhamy, M. Wollner, A. Peer, G. Bar-Sela, 1545PD – The effect of cannabis use on tumor response to nivolumab in patients with advanced malignancies, Annals of Oncology, Volume 28, Supplement 5, 2017, Page v544, ISSN 0923-7534, https://doi.org/10.1093/annonc/mdx388.005.
-
Yamaori S, Koeda K, Kushihara M, Hada Y, Yamamoto I, Watanabe K. Comparison in the in vitro inhibitory effects of major phytocannabinoids and polycyclic aromatic hydrocarbons contained in marijuana smoke on cytochrome P450 2C9 activity. Drug Metab Pharmacokinet. 2012 ;27(3) :294-300. Doi : 10.2133/dmpk.dmpk-11-rg-107. Epub 2011 Dec 13. PMID : 22166891.
-
Damkier P, Lassen D, Christensen MMH, Madsen KG, Hellfritzsch M, Pottegård A. Interaction between warfarin and cannabis. Basic Clin Pharmacol Toxicol. 2019 Jan ;124(1) :28-31. Doi : 10.1111/bcpt.13152. Epub 2018 Nov 6. PMID : 30326170.
-
Hsu A, Painter NA. Probable Interaction Between Warfarin and Inhaled and Oral Administration of Cannabis. J Pharm Pract. 2020 Dec;33(6):915-918. Doi: 10.1177/0897190019854958. Epub 2019 Jul 18. PMID: 31319733.
-
Stoll AL, Cole JO, Lukas SE. A case of mania as a result of fluoxetine-marijuana interaction. J Clin Psychiatry. 1991 Jun;52(6):280-1. PMID: 1647392.
-
Vierke C, Marxen B, Boettcher M, Hiemke C, Havemann-Reinecke U. Buprenorphine-cannabis interaction in patients undergoing opioid maintenance therapy. Eur Arch Psychiatry Clin Neurosci. 2021 Aug ;271(5) :847-856. Doi : 10.1007/s00406-019-01091-0. Epub 2020 Jan 6. PMID: 31907614; PMCID: PMC8236049.
-
Mackie J, Clark D. Cannabis toxic psychosis while on disulfiram. Br J Psychiatry. 1994 Mar;164(3):421. Doi: 10.1192/bjp.164.3.421a. PMID: 8199803. Geffrey AL, Pollack SF, Bruno PL, Thiele EA. Drug-drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Epilepsia. 2015 Aug;56(8):1246-51. Doi: 10.1111/epi.13060. Epub 2015 Jun 26. PMID: 26114620.
-
Lacoursiere RB, Swatek R. Adverse interaction between disulfiram and marijuana : a case report. Am J Psychiatry. 1983 Feb;140(2):243-4. Doi: 10.1176/ajp.140.2.243. PMID: 6295192.
-
Arellano AL, Papaseit E, Romaguera A, Torrens M, Farré M. Neuropsychiatric and General Interactions of Natural and Synthetic Cannabinoids with Drugs of Abuse and Medicines. CNS Neurol Disord Drug Targets. 2017;16(5):554-566. Doi: 10.2174/1871527316666170413104516. PMID: 28412920.
Name/acronym/symbol
Coke/C/crack/snow/Charlie/nose candy/blow/bump/sugar/white powder/crack/base/rock/stones
Form and method of administration
White powder / Yellow stone for crack
Nasal/Smoked/Intravenous
Pharmacokinetic properties
Cocaine is absorbed from all sites of application, including mucous membranes and gastrointestinal mucosa. By oral or
intra-nasal route, 60 to 80% of cocaine is absorbed.
CYP450 3A4 is involved in cocaine N-demethylation. Into norcocaine, active hepatotoxic metabolite.
Half-life : from 10 minutes in IV to 1 hour when snorted
| 3A4 | |
|---|---|
| Substrate | X |
Unknown if cocaine is a major or a minor substrate of CYP450 3A4.
In the presence of alcohol, a further active metabolite, cocaethylene is formed, and is more toxic then cocaine itself.
Pharmacodynamic properties
Cocaine binds differentially to the dopamine, serotonin, and norepinephrine transport proteins and directly prevents the re-uptake of dopamine, serotonin,
and norepinephrine into pre-synaptic neurons.
Dose-related increases in heart rate, blood pressure, and pupil diameter.
Recommendations :
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Serotonin reuptake inhibitors, fentanyl, lamotrigine, aripiprazole | Risk of serotoninergic syndrom. | High | Not recommended. Clinical monitoring | |
| Ethanol | Enhanced hepatotoxicity and cardio-vascular risks | High | Not recommended. | |
| CYP3A4 inhibitors | Increased cocaine plasma levels. Risk of increased cardiovascular toxicity | Reduced cocaine plasma levels. Increased norcocaine plasma levels. Risk of increased hepatotoxicity | Moderate | Not recommended. Clinical/pharmacological monitoring. Reduced dosages if associated. |
| CYP 3A4 inducers | Increased norcocaine plasma levels. Risk of increased hepatotoxicity | Increased cocaine plasma levels. Risk of increased cardiovascular toxicity | Moderate | Not recommended. Clinical/pharmacological monitoring. |
| Tricyclic antidepressants | Diminish the vasoconstrictive effects of cocaine and are cardioprotective in rats. Risk of serotoninergic syndrom | Moderate | Clinical monitoring | |
| Beta blockers | Fatal interactions have been reported, along with propranolol induced-hypertension. | Moderate | Clinical monitoring. Consider substitution by calcium-channel blockers as they may be cardioprotective. | |
| Flupenthixol | May decrease cocaine craving. | Moderate | - | |
| Clozapine | Most effective antipsychotic for reducing cocaine abuse among patients with schizophrenia. But also induces dose-dependent development of cardiovascular toxicity | Moderate | - | |
| Calcium channel blockers | May be cardioprotective in cocaine use. | Low | May be preferred as anti-hypertensive drug in cocaine-users. | |
| Ziprasidone | Increased cocaine toxicity with long duration treatment | Low | Clinical monitoring | |
| Monoamine oxidase B inhibitors (MAO-B). | May augment the pressor effect of sympathomimetic amines. Reduces cocaine cardiotoxicity | Uncategorized |
- https ://go.drugbank.com/drugs/DB00907
-
McCance EF, Price LH, Kosten TR, Jatlow PI. Cocaethylene: pharmacology, physiology and behavioral effects in humans. J Pharmacol Exp Ther. 1995 Jul;274(1):215-23. PMID: 7616402.
- https://americanaddictioncenters.org/cocaine-treatment/differences-with-crack
-
Sands B; Ciraulo A, Cocaine Drug-Drug Interactions. Journal of Clinical Psychopharmacology 12(1):p 49-55, February 1992.
-
Guinn MM, Bedford JA, Wilson MC. Antagonism of intravenous cocaine lethality in nonhuman primates. Clin Toxicol 1980; 16(4): 499-508.
-
Catravas JD, Waters IW. Acute cocaine intoxication in the con- scious dog: Studies on the mechanism of lethality. J Pharmacol Exp Ther 1981; 217(2): 350-6.
-
Ramoska E, Sacchetti AD. Propranolol-induced hypertension in treatment of cocaine intoxication. Ann Emerg Med 1985; 14(11): 1112-3.
-
Gallelli L, Gratteri S, Siniscalchi A, Cione E, Sirico S, Seminara P, Caroleo MC, De Sarro G. Drug-Drug Interactions in Cocaine-users and their Clinical Implications. Curr Drug Abuse Rev. 2017;10(1):25-30. doi: 10.2174/1874473710666170920143344. PMID: 29185916.
Name/acronym/symbol
Keta/special K/ket
Form and method of administration
Liquid/Powder
Nasal/ IV
Pharmacokinetic properties
Major metabolisation by 3A4
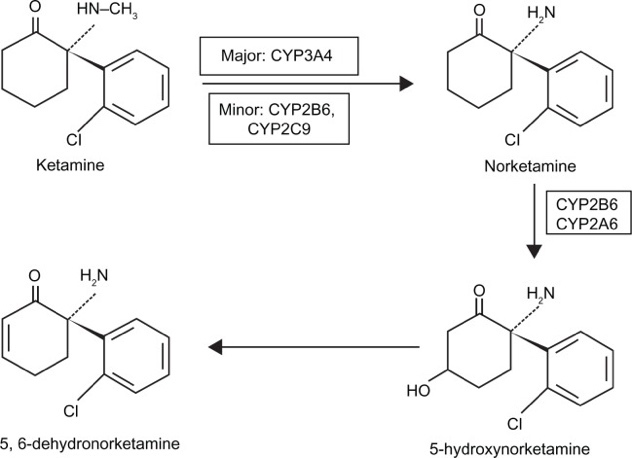
Minor metabolization by 2B6 and 2C9
3A4 : Low affinity/High capacity enzyme
2B6 : High affinity/Low capacity enzyme
| 2B6 | 2C9 | 3A4 | |
|---|---|---|---|
| Substrate |
| Major metabolic pathway / potent inhibitor-inducer | |
|---|---|
| Minor metabolic pathway / moderate inhibitor-inducer |
The CYP2B6*6 allele is the most common polymorphism and is found mostly in African, African-American, and some Asian populations. CYP2B6*6 activity is reduced compared to others CYP2B6 alleles. These populations may require lower doses of ketamine.
Pharmacodynamic properties
Non-competitive antagonism of NDMA receptor
Non-barbiturate general anesthetic, fast-acting, inducing dissociative anesthesia.
This anesthetic state is characterized by:
Deep and prolonged anesthesia,
Loss of consciousness, more akin to patient disconnection than genuine sleep,
Preservation of pharyngeal and laryngeal reflexes,
Maintenance or subtle increase in muscle tone,
Typically, cardiovascular and respiratory stimulation.
Recommendations :
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| 3A4 inhibitors | Increased plasma levels which may increase toxicity. | Reduced plasma levels why may decrease medication efficacy | Moderate | Not recommended. Clinical/pharmacological monitoring if associated. Reduced dosages if associated. |
| 3A4 inducers | Reduced plasma levels why may decrease medication efficacy. | Increased plasma levels which may increase toxicity. | Moderate | Not recommended. Clinical/pharmacological monitoring if associated. Increased dosages may be recommended. |
| Benzodiazepines | May reduce ketamine antidepressant activity | Moderate | ||
| Lamotrigine | May reduce the occurrence of ketamine adverse effects | Moderate | ||
| 2B6/2C9 inhibitors | Increased plasma levels which may increase toxicity. | Reduced plasma levels why may decrease medication efficacy | Low | Clinical/pharmacological monitoring if associated. |
| 2B6/2C9 inducers | Reduced plasma levels why may decrease medication efficacy | Increased plasma levels which may increase toxicity. | Low | Clinical/pharmacological monitoring if associated. |
| Anti-depressants | No interaction observed | May be compatible |
-
Hijazi Y, Boulieu R. Contribution of CYP3A4, CYP2B6, and CYP2C9 isoforms to N-demethylation of ketamine in human liver microsomes. Drug Metab Dispos. 2002 Jul;30(7):853-8. doi: 10.1124/dmd.30.7.853. PMID: 12065445.
-
Bergman SA. Ketamine: review of its pharmacology and its use in pediatric anesthesia. Anesth Prog. 1999 Winter;46(1):10-20. PMID: 10551055; PMCID: PMC2148883.
-
Andrade C. Ketamine for Depression, 5: Potential Pharmacokinetic and Pharmacodynamic Drug Interactions. J Clin Psychiatry. 2017 Jul;78(7):e858-e861. doi: 10.4088/JCP.17f11802. PMID: 28858450.
- http://agence-prd.ansm.sante.fr/php/ecodex/rcp/R0293746.htm
- https://sofia.medicalistes.fr/spip/IMG/pdf/ketamine-2.pdf
-
Li, Jih-Heng & Vicknasingam, Balasingam & Cheung, Yuet-Wah & Zhou, Wang & Nurhidayat, Adhi & Des Jarlais, Don & Schottenfeld, Richard. (2011). To use or not to use: an update on licit and illicit ketamine use. Substance abuse and rehabilitation. 2. 11-20. 10.2147/SAR.S15458.
Name/acronym/symbol
Heroin : Big H/brown sugar/junk
Methadone : Meta
Buprenorphine : Subu
Form and method of administration
Ingested, snorted, IV
Pharmacokinetic properties
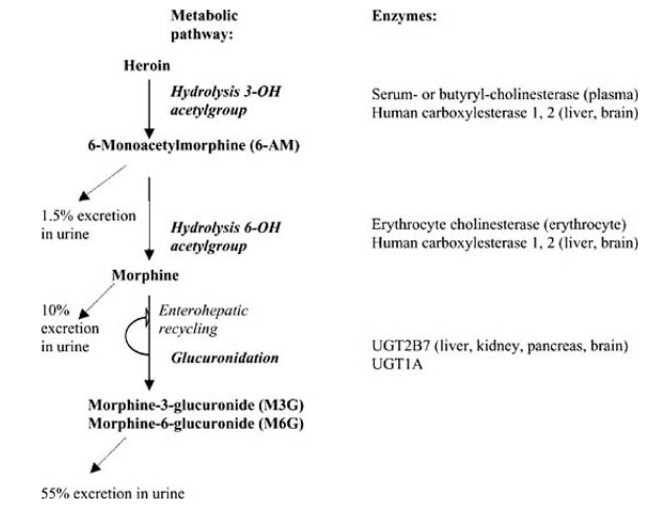
Heroine (diacetyl-morphine)
Major renal metabolism
Morphine and M-6G are major substrates of P-gp
Methadone
Major substrate 2B6, 3A4, P-gp
Minor substrate 1A2, 2C19, 2D6
Strong inhibitor of P-gp
Moderate inhibitor of 2D6
| Methadone | 1A2 | 2B6 | 2C19 | 2D6 | 3A4 | P-gp |
|---|---|---|---|---|---|---|
| Substrate | ||||||
| Inhibitor |
Buprenorphine
Minor substrate 3A4
| 3A4 | |
|---|---|
| Substrate |
| Major metabolic pathway / potent inhibitor-inducer | |
|---|---|
| Minor metabolic pathway / moderate inhibitor-inducer |
Pharmacodynamic properties
Heroine, methadone :
Pure μ receptor agonist
Buprenorphine :
Partial μ receptor agonist
Recommendations :
HEROIN/MORPHIN
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Ethanol | Increased 6-AM levels by inhibition of carboxylesterases. Enhanced risk for overdose | Reduced 6-AM levels | High | Do not associate. Lethal risk. |
| Cocaine | Competitive inhibition on carboxylesterases. | - | High | Clinical/pharmacological monitoring. Reduced heroin/cocain dosage may be adapted to the patient. |
| P-gp inhibitors | Increased morphin levels levels which may increase toxicity. | Reduced morphin levels which may decrease medication efficacy. | Moderate | Clinical/pharmacological monitoring. Reduced morphin dosage may be adapted to the patient. |
| P-gp inducers | Reduced morphin levels levels which may decrease medication efficacy. | Increased morphin levels which may increase toxicity | Moderate | Clinical/pharmacological monitoring. Dosage should be adjusted accordingly. |
| Central nervous system depressants | Synergism. Risk of respiratory depression | Moderate | Clinical monitoring. Dosage should be adjusted accordingly. | |
| Oxazepam, chloramphenicol, tricyclic antidepressants, ranitidine | Competitive inhibition of glucuronidation to morphine 3-glucuronide (M3G) and morphine 6-glucuronide (M6G) Enhanced opioids effect | Low | Clinical/pharmacological monitoring. Reduced heroin dosage may be adapted to the patient. |
METHADONE
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Agonist-antagonist opioids | Reduced analgesic effect due to competitive receptor blockade, with risk of withdrawal syndrome. | - | High | Contra-indicated |
| Naltrexone | Risk of withdrawal syndrome. | - | High | Contra-indicated |
| Sultopride | Increased risk of ventricular rhythm disorders, particularly torsades de pointe. | - | High | Contra-indicated |
| Class Ia antiarrhythmics (quinidine, hydroquinidine, disopyramide), class III antiarrhythmics (amiodarone, dofetilide, ibutilide, sotalol), certain neuroleptics (amisulpride, chlorpromazine, cyamemazine, droperidol, haloperidol, levomepromazine, pimozide, sulpiride, thioridazine, tiapride, veralipride) except sultopride (see Contraindicated associations), certain antiparasitic agents (halofantrine, lumefantrine, pentamidine), certain macrolides (azithromycin, clarithromycin, roxithromycin, erythromycin IV, spiramycin IV), bepridil, cisapride, diphemanil, mizolastine, moxifloxacin, vincamine IV | Increased risk of QT interval prolongation and ventricular rhythm disorders, particularly torsades de pointe. | - | High | Not recommended. Clinical and electrocardiogram monitoring |
| Ethanol | increases the sedative effect of morphine analgesics. | High | Not recommended | |
| 2B6/3A4/P-gp inhibitors | Increased plasma levels which may increase toxicity. | Reduced plasma levels which may decrease medication efficacy. | High | Not recommended. Clinical/pharmacological monitoring and reduced dosage may be adapted to the patient. |
| 2B6/3A4/P-gp inducers | Reduced plasma levels which may decrease medication efficacy. | Increased plasma levels which may increase toxicity. | High | Not recommended. Clinical/pharmacological and increased dosage may be adapted to the patient |
| P-gp substrates | Increased substrates plasma levels which may increase toxicity | Reduced substrate plasma levels why may decrease substrates efficacy. | High | Not recommended. Clinical pharmacological monitoring and reduced substrate dosage may be adapted to the patient. |
| Bisoprolol, carvédilol, métoprolol, nebivolol, bradycardic drugs, hypokalemic drugs | Increased risk of ventricular rhythm disorders, particularly torsades de pointe | High | Precaution for use. Clinical and electrocardiogram monitoring | |
| Cimétidine (> 800mg/day), fluvoxamine | Increased methadone plasma concentrations with overdose and increased risk of QT interval prolongation and ventricular rhythm disorders, including torsades de pointe. | High | Precaution for use. Enhanced clinical and electrocardiographic monitoring: if necessary, adjustment of methadone dosage during treatment with cimetidine and after its discontinuation. | |
| Central nervous system depressants | Increased risk of respiratory depression | High | To take in account | |
| Cocaïne | Increased metabolism. Reduced plasma levels which may decrease medication efficacy. | Increased plasma levels which may increase toxicity | Moderate | Increased dosage may be adapted to the patient |
| 1A2/2C19/2D6 inhibitors | Increased plasma levels which may increase toxicity. | Reduced plasma levels why may decrease medication efficacy. | Moderate | Clinical/pharmacological monitoring if associated. |
| 1A2/2C19/2D6 inducers | Reduced plasma levels why may decrease medication efficacy. | Increased plasma levels which may increase toxicity. | Moderate | Clinical/pharmacological monitoring if associated. |
BUPRENORPHINE
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| Methadone | Decreased effect of methadone due to competitive receptor blockade, with risk of withdrawal syndrome. | High | Contra-indicated | |
| Level III opioids analgesics | Reduction in the analgesic effect of the morphine may be observed, due to competitive receptor blockade, with the risk of a withdrawal syndrome. | High | Contra-indicated | |
| Central nervous system depressants | Increased risk of respiratory depression | High | To take in account | |
| 3A4 inhibitors | Increased plasma levels | Reduced plasma levels | Moderate | Enhanced clinical monitoring with strong 3A4 inhibitors. Reduced buprenorphine dosage may be necessary. |
| 3A4 inducers | Reduced plasma levels | Increased plasma levels | Moderate | Clinical monitoring. |
| Protease inhibitors | Risk of increasing or decreasing the effects of buprenorphine : withdrawal symptom or overdose | Moderate | Enhanced clinical monitoring .Reduced buprenorphine dosage may be necessary. |
- https://www.hug.ch/sites/interhug/files/structures/pharmacologie_et_toxicologie_cliniques/a5_cytochromes_6_2.pdf
-
Rook EJ, Huitema AD, van den Brink W, van Ree JM, Beijnen JH. Pharmacokinetics and pharmacokinetic variability of heroin and its metabolites: review of the literature. Curr Clin Pharmacol. 2006 Jan;1(1):109-18. doi: 10.2174/157488406775268219. PMID: 18666382.
-
McCance-Katz EF, Sullivan LE, Nallani S. Drug interactions of clinical importance among the opioids, methadone and buprenorphine, and other frequently prescribed medications: a review. Am J Addict. 2010 Jan-Feb;19(1):4-16. doi: 10.1111/j.1521-0391.2009.00005.x. PMID: 20132117; PMCID: PMC3334287.
- http://agence-prd.ansm.sante.fr/php/ecodex/rcp/R0249836.htm
- http://agence-prd.ansm.sante.fr/php/ecodex/rcp/R0223085.htm
-
Kharidia, J., Howgate, E.M., Laffont, C.M., Liu, Y. and Young, M.A. (2021), Evaluation of Drug-Drug Interaction Liability for Buprenorphine Extended-Release Monthly Injection Administered by Subcutaneous Route. Clinical Pharmacology in Drug Development, 10: 1064-1074. https://doi.org/10.1002/cpdd.934
Name/acronym/symbol
Shrooms/Mushies/magics/philosopher’s stones
Form and method of administration
Ingested
Pharmacokinetic properties
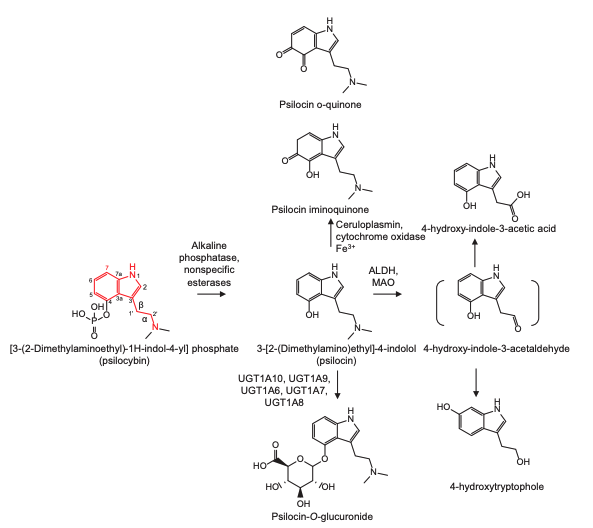
Main enzymes involved in psylocibin metabolism :
Alkaline phosphatase
UGT1A10
UGT1A9
Aldehyde dehydrogenase
MAO-A
There are few pharmacologic agents that influence UGT1A9 and UGT1A10
Furthermore, the pharmacokinetics of psilocin, the active metabolite of psilocybin, is linear and is minimally affected by renal clearance
Pharmacodynamic properties
Serotonin 5HT-2A receptor agonist
Metabolized into active metabolite : psilocin by alkaline phosphatase or non-specific esterases
Mild increases in blood pressure and heart rate
Increased sense of unity, transcendence of time and space, loss of self, and euphoria UGT
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| MAO-A inhibitors Moclobemide, iproniazide | Increased psilocin levels | Reduced plasma levels | Moderate | Clinical/pharmacological monitoring. Reduced dosage may be adapted to the patient. |
| 5HT2A blockers | Antagonism. Attenuation of psilocybin’s effects | Low | Should be taken in account if associated. | |
| Selective serotonin reuptake inhibitors | Antagonism. Reduction of the negative effects of psilocybin (subjective bad drug effects, anxious-ego dissolution, anxiety) | Low | Clinical monitoring if associated. | |
| Inhibitors/inducers of UGT 1A9/1A10 enzymes | Increased/reduced psilocin plasma levels | Low | Concurrent use should be avoided |
-
Sarparast A, Thomas K, Malcolm B, Stauffer CS. Drug-drug interactions between psychiatric medications and MDMA or psilocybin: a systematic review. Psychopharmacology (Berl). 2022 Jun;239(6):1945-1976. doi: 10.1007/s00213-022-06083-y. Epub 2022 Mar 7. PMID: 35253070; PMCID: PMC9177763.
-
Holze, F., Becker, A.M., Kolaczynska, K.E., Duthaler, U. and Liechti, M.E. (2023), Pharmacokinetics and Pharmacodynamics of Oral Psilocybin Administration in Healthy Participants. Clin Pharmacol Ther, 113: 822-831. https://doi.org/10.1002/cpt.2821
-
Dinis-Oliveira RJ. Metabolism of psilocybin and psilocin: clinical and forensic toxicological relevance. Drug Metab Rev. 2017 Feb;49(1):84-91. doi: 10.1080/03602532.2016.1278228. Epub 2017 Jan 31. PMID: 28074670.
Name/acronym/symbol
MD/speed/uppers/molly
Form and method of administration
Ingested
Pharmacokinetic properties
Main enzymes involved in méthylènedioxyméthamphétamine (MDMA) metabolism
CYP2D6 (auto inhibitor)
CYP3A4
CYP2B6
CYP2C19
CYP1A2
| 2D6 | 3A4 | 1A2/2B6/2C19 | |
|---|---|---|---|
| Substrates |
| Major metabolic pathway / potent inhibitor-inducer | |
|---|---|
| Minor metabolic pathway / moderate inhibitor-inducer |
Pharmacodynamic properties
Inhibit the reuptake of serotonin (5-HT), to facilitate serotonin release, and to a lesser extent cause dopamine and noradrenaline.
MDMA acute adverse effects may include increased heart rate and blood pressure, tremor, sweating, bruxism, and life-threatening hyperthermia that may be further complicated by rhabdomyolysis, disseminated intravascular coagulation, and acute renal failure.
Recommendations :
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| MAO inhibitors Moclobemide, linezolide .. | Synergism. Serotoninergic syndrome | High | Avoid association. | |
| Pro-serotoninergic Drugs | Synergism. Serotoninergic syndrome | High | Avoid association. | |
| 2D6 / 3A4 inhibitors | Increased plasma levels which may increase toxicity | Reduced plasma levels which may decrease psychoactive effects | Moderate | Not recommended. Clinical monitoring and reduced dosages if associated |
| 2D6 / 3A4 inducers | Reduced plasma levels which may decrease psychoactive effects | Increased plasma levels which may increase toxicity | Moderate | Not recommended. Clinical monitoring if associated |
| 1A2/2B6/2C19 inhibitors | Increased plasma levels which may increase toxicity | Reduced plasma levels which may decrease psychoactive effects | Low | Clinical monitoring |
| 1A2/2B6/2C19 inducers | Reduced plasma levels which may decrease psychoactive effects | Increased plasma levels which may increase toxicity | Low | Clinical monitoring |
-
Sarparast A, Thomas K, Malcolm B, Stauffer CS. Drug-drug interactions between psychiatric medications and MDMA or psilocybin: a systematic review. Psychopharmacology (Berl). 2022 Jun;239(6):1945-1976. doi: 10.1007/s00213-022-06083-y. Epub 2022 Mar 7. PMID: 35253070; PMCID: PMC9177763.
-
Jessica R. Oesterheld, Scott C. Armstrong, Kelly L. Cozza, Ecstasy: Pharmacodynamic and Pharmacokinetic Interactions(2),Psychosomatics, Volume 45, Issue 1, 2004, Pages 84-87, ISSN 0033-3182, https://doi.org/10.1176/appi.psy.45.1.84.
-
Papaseit E, Vázquez A, Pérez-Mañá C, Pujadas M, de la Torre R, Farré M, Nolla J. Surviving life-threatening MDMA (3,4-methylenedioxymethamphetamine, ecstasy) toxicity caused by ritonavir (RTV). Intensive Care Med. 2012 Jul;38(7):1239-40. doi: 10.1007/s00134-012-2537-9. Epub 2012 Mar 30. PMID: 22460853.
Name/acronym/symbol
LSD/acid/doses/dots/trips/window pane
Form and method of administration
Liquid, ingested
Pharmacokinetic properties
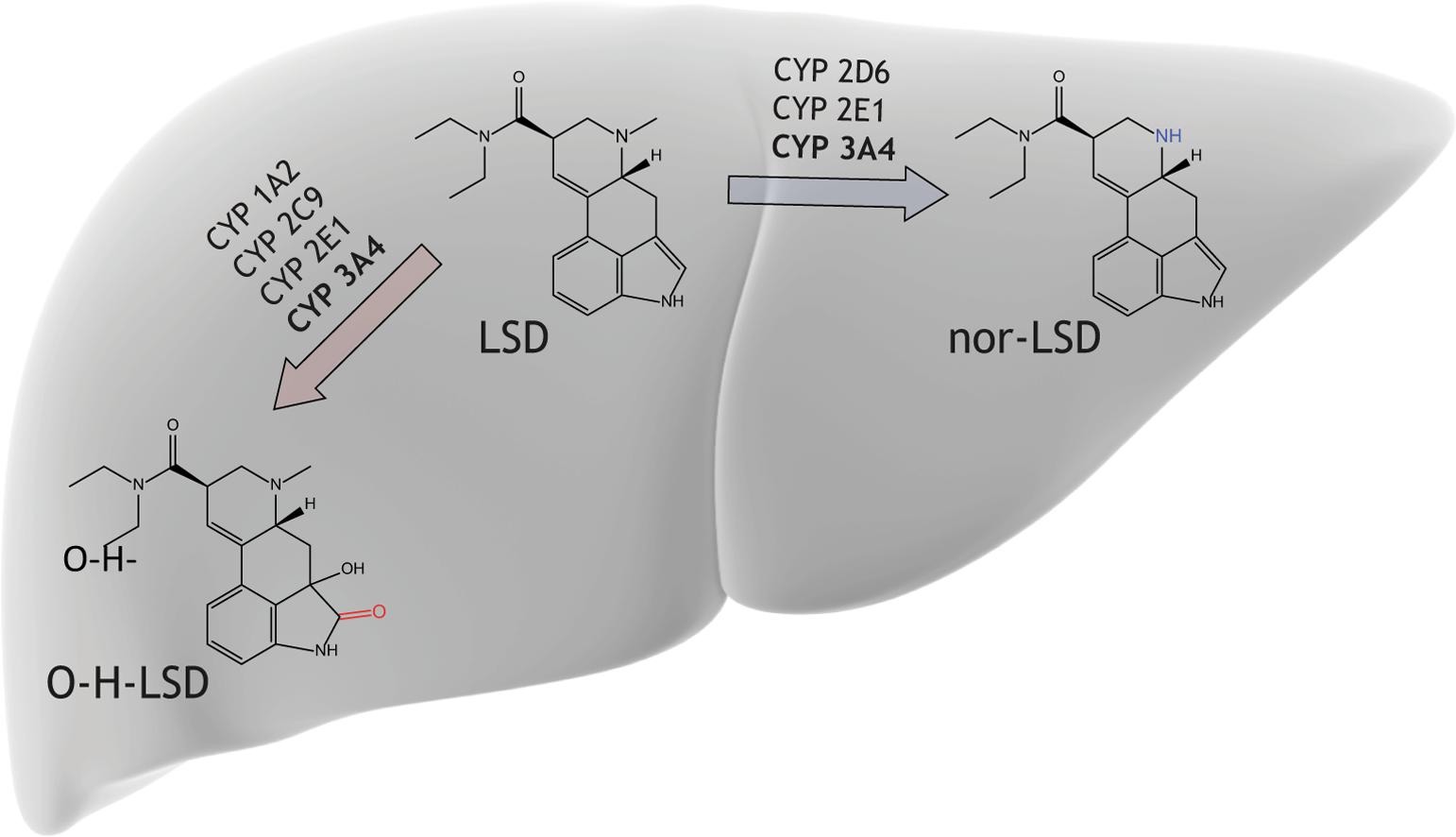
O-H-LSD may not have psychedelic properties in vivo
| 2C9 / 2D6 / 2E1 | 1A2 / 3A4 | |
|---|---|---|
| Substrates |
| Major metabolic pathway / potent inhibitor-inducer | |
|---|---|
| Minor metabolic pathway / moderate inhibitor-inducer |
Pharmacodynamic properties
High affinity for serotoninergic (5-HT1A/B and 5HT2A) and also dopaminergic (D1-D5) receptors. Psychedelic effects
| Drug(s) | Nature of interaction | Change with smoking cessation | Clinical importance | Advice(s) |
|---|---|---|---|---|
| 1A2 / 3A4 inhibitors | Increased LSD plasma levels which may increase psychoactive effects | Reduced LSD plasma levels which may decrease psychoactive effects | High | Not recommended. |
| Lithium | Synergism. Earlier onset, increased hallucinatory and psychological effects of LSD | High | Not recommended. | |
| Reserpine | Synergism. Enhanced LSD effects | High | Not recommended. | |
| 1A2 / 3A4 inducers | Reduced LSD plasma levels which may decrease psychoactive effects | Increased LSD plasma levels which may increase psychoactive effects | Moderate | Precaution for use |
| Chlorpromazine | Synergism/antagonism on dopaminergic receptors. Psychoactive effects may be reduced or enhanced. Unclear data | Moderate | Not recommended. | |
| MDMA | Longer Psychedelic experience (+ 1.5 h) Increased blood pressure and heart rate | Moderate | Not recommended | |
| Niacin (B3 vitamin) | Pre-LSD ingestion : Delayed onset of LSD effects Post LSD ingestion : Might attenuate all LSD effect | Moderate | Precaution for use | |
| 2C9 / 2D6 / 2E1 inhibitors | Increased plasma levels which may increase toxicity | Reduced plasma levels which may decrease psychoactive effects | Moderate | Clinical monitoring |
| 2B6/2C19 inducers | Reduced plasma levels which may decrease psychoactive effects | Increased plasma levels which may increase toxicity | Moderate | Clinical monitoring |
| MAO inhibitors | Might attenuate LSD effects. Unclear data | Low | Clinical monitoring | |
| Ethanol | Might reduce Ethanol effects. No alteration of LSD effects | Low |
-
1.
Halman A, Kong G, Sarris J, Perkins D. Drug-drug interactions involving classic psychedelics: A systematic review. Journal of Psychopharmacology. 2024;38(1):3-18. doi:10.1177/02698811231211219 -
Halberstadt AL, Geyer MA. Multiple receptors contribute to the behavioral effects of indoleamine hallucinogens. Neuropharmacology. 2011 Sep;61(3):364-81. doi: 10.1016/j.neuropharm.2011.01.017. Epub 2011 Jan 20. PMID: 21256140; PMCID: PMC3110631.
-
Dino Luethi, Marius C. Hoener, Stephan Krähenbühl, Matthias E. Liechti, Urs Duthaler,
Cytochrome P450 enzymes contribute to the metabolism of LSD to nor-LSD and 2-oxo-3-hydroxy-LSD: Implications for clinical LSD use,
Biochemical Pharmacology,
Volume 164,
2019,
Pages 129-138,
ISSN 0006-2952,
https://doi.org/10.1016/j.bcp.2019.04.013